Technological innovations in blood-contact medical devices have reshaped the landscape of modern medicine, enabling numerous life-saving medical interventions such as cardiac surgery and long-term vascular access. However, these products generally face a core challenge: once the artificial materials come into contact with blood, the body's clotting mechanism is rapidly activated. Therefore, the anticoagulation problem has always been a critical technological barrier that needs to be overcome in the research and manufacturing of medical devices.
Blood is far more than a fluid — it is a living tissue saturated with cells, proteins, and signaling molecules. When it encounters a foreign material, the consequences escalate quickly.
Within seconds of surface contact, plasma proteins — including fibrinogen, von Willebrand factor, and immunoglobulin G — coat the foreign material in what amounts to a molecular welcome party nobody asked for. This process, known as protein adsorption, is the first triggering step in device-induced thrombosis.
Activation of Factor XII on negatively charged surfaces initiates the intrinsic coagulation pathway, while exposure of tissue factor activates the extrinsic pathway. Both pathways activate Factors V and VIII, generating a thrombin burst that converts fibrinogen to fibrin, forming a stable clot structure.
Natural anticoagulant substances maintain equilibrium within this system. Antithrombin III (ATIII), when bound to heparin, neutralizes thrombin and Factor Xa with remarkable efficiency — approximately 1,000-fold acceleration. Protein C and Protein S provide an additional layer of control by cleaving and inactivating activated coagulation factors to limit the clotting process.
Blood-contacting devices create surfaces that bypass or overwhelm these regulatory mechanisms. This is precisely why artificial anticoagulation strategies are necessary.
In vascular stents, acute thrombosis can completely occlude a vessel, leading to myocardial infarction or stroke. In cardiopulmonary bypass circuits, circuit thrombosis can release emboli into the arterial circulation, causing distal organ damage. In dialysis catheters, thromb formation leads to reduced blood flow and treatment interruptions.
Beyond acute events, subclinical thrombosis drives chronic complications. Neointimal hyperplasia — the proliferation of smooth muscle cells and extracellular matrix within the subendothelial layer — is the primary mechanism of in-stent restenosis, with platelet-derived growth factor as a key driver of this process.
Thrombus on device surfaces also serves as a nidus for infection. Bacteria thrive in protein-rich thrombotic matrices. Infected thrombi are exceedingly difficult to treat with antibiotics alone.
From an economic perspective, device-related thrombosis affects every stakeholder. Patients endure prolonged hospital stays and potential re-interventions. Clinicians face complex management decisions. Healthcare systems bear significantly increased treatment costs. This is why surface modification technologies — such as heparin coating — have become indispensable. Not optional. Essential.
Heparin is a sulfated glycosaminoglycan found in mast cells and basophils throughout the body. Clinically, heparin has been in use since the 1930s and remains one of the most widely used parenteral anticoagulant agents.
The critical element: heparin contains a unique pentasaccharide sequence that binds to antithrombin III (ATIII) with high affinity. This binding induces a conformational change in ATIII, accelerating its inhibition of thrombin (Factor IIa) and Factor Xa by approximately 1,000-fold.
Other coagulation factors — IXa, XIa, XIIa — are also inhibited through this mechanism, albeit with varying efficiencies.
An important detail: the heparin chain must be at least 18 sugar units long to simultaneously bind ATIII and thrombin. Shorter chains can accelerate Factor Xa inhibition but cannot directly inhibit thrombin.
When heparin is immobilized on a surface rather than administered systemically, this catalytic mechanism generates a localized anticoagulant effect — preventing thrombosis at the device surface without requiring systemic anticoagulation.
The heparin–ATIII interaction is one of the most extensively studied molecular recognition events in biology. Understanding it at the molecular level directly informs coating design.
ATIII is a 58 kDa serine protease inhibitor. Under normal conditions, it inhibits thrombin and other coagulation factors through a slow, stepwise mechanism. Heparin binding induces an allosteric change that exposes the reactive center loop of ATIII, enabling rapid thrombin capture.
The binding site on ATIII involves specific arginine and lysine residues in the D-helix region. These positively charged residues interact with the negatively charged sulfate groups on the heparin chain. This charge complementarity renders the binding both highly affine and specific.
For surface immobilization, this charge-based interaction presents both opportunities and challenges. Preserving the critical pentasaccharide sequence and ensuring adequate chain flexibility are non-negotiable requirements.
Surface-bound heparin aims to achieve local anticoagulation without producing significant systemic effects. The key requirement is that immobilized heparin must retain biological activity.
This concept was established through pioneering work in the 1960s and 1970s, followed by clinical applications in cardiac surgery and expansion into vascular devices, dialysis equipment, extracorporeal life support systems, and long-term implants.
A critical distinction: systemically administered heparin distributes throughout the entire intravascular volume. Surface-bound heparin resides at the blood–device interface, where local concentration is extremely high but systemic exposure is minimal.
How heparin attaches to a device surface fundamentally influences coating durability, bioactivity retention, and clinical performance. Two primary strategies dominate: ionic bonding and covalent bonding.
Ionic bonding relies on electrostatic attraction between positively charged surface sites and negatively charged heparin molecules. Many surface preparation methods create amine groups that bind heparin through electrostatic interactions. This approach is relatively straightforward and cost-effective, making it suitable for short-term applications.
However, ionic coatings have notable limitations. Electrostatic interactions are reversible — variations in ionic strength, pH, or competitive binding can all cause heparin elution. In vivo, heparin may gradually release from the surface over time, diminishing anticoagulant efficacy and potentially causing systemic effects.
Covalent bonding involves chemical reactions between heparin and functional groups on the device surface, producing bonds that are orders of magnitude more stable than ionic interactions. Typical methods include carbodiimide chemistry, Schiff base formation, or click chemistry.
Covalent attachment ensures coating stability under physiological conditions. This stability is critical for long-term implants, where coating integrity must be maintained for months or years.
The trade-off: if the bonding reaction disrupts the critical pentasaccharide sequence or restricts heparin chain flexibility, bioactivity loss may result. Successful covalent coating methods must strike a balance between stable attachment and functional preservation.
This is where things get interesting. Advanced covalent coating strategies focus on maintaining heparin bioactivity while achieving durable attachment. Endpoint attachment methods are particularly significant.
Conventional covalent attachment typically involves random crosslinking through multiple heparin functional groups. This creates a highly crosslinked network that immobilizes heparin molecules in a compressed conformation, significantly reducing their ability to interact with ATIII.
Endpoint covalent attachment specifically targets a single functional group at one end of the heparin molecule, leaving the remainder of the chain free to interact with ATIII. This approach maximizes heparin bioavailability while maintaining attachment durability.
jMedtech's approach embodies this strategy. By leveraging proprietary endpoint attachment chemistry, the jHemo PC® platform achieves high-density heparin immobilization while preserving molecular flexibility for optimal anticoagulant function.
Endpoint attachment also offers advantages in coating uniformity and reproducibility. By controlling the orientation of immobilized heparin molecules — consistently presenting ATIII binding sites outward toward the blood — maximum anticoagulant activity per unit surface area is achieved.
The choice of bonding method directly impacts clinical outcomes. Surface stability, anticoagulant efficacy, safety, device performance — all depend on how heparin is attached.
Clinically, the most concerning issue with ionic bonding is coating instability. Case reports and clinical studies have documented heparin elution leading to systemic anticoagulant effects and variable performance. These instabilities have driven many manufacturers toward covalent methods.
Manufacturing considerations also favor covalent approaches. Ionic coatings are sensitive to surface preparation variability and environmental conditions, making quality control more challenging. Covalent methods generally deliver more reproducible results and wider process windows.
For manufacturers navigating varying regulatory requirements across global markets, the well-documented stability and performance of covalent heparin coatings provide a more robust foundation for regulatory submissions.
The primary function of heparin coatings is straightforward: prevent thrombosis on blood-contacting surfaces. Antithrombogenicity is achieved through multiple complementary mechanisms.
The ATIII-dependent mechanism is the most significant. Surface-bound heparin captures circulating ATIII, accelerating the inhibition of thrombin and Factor Xa at the blood–device interface. This localized action prevents thrombus formation without requiring systemic anticoagulation.
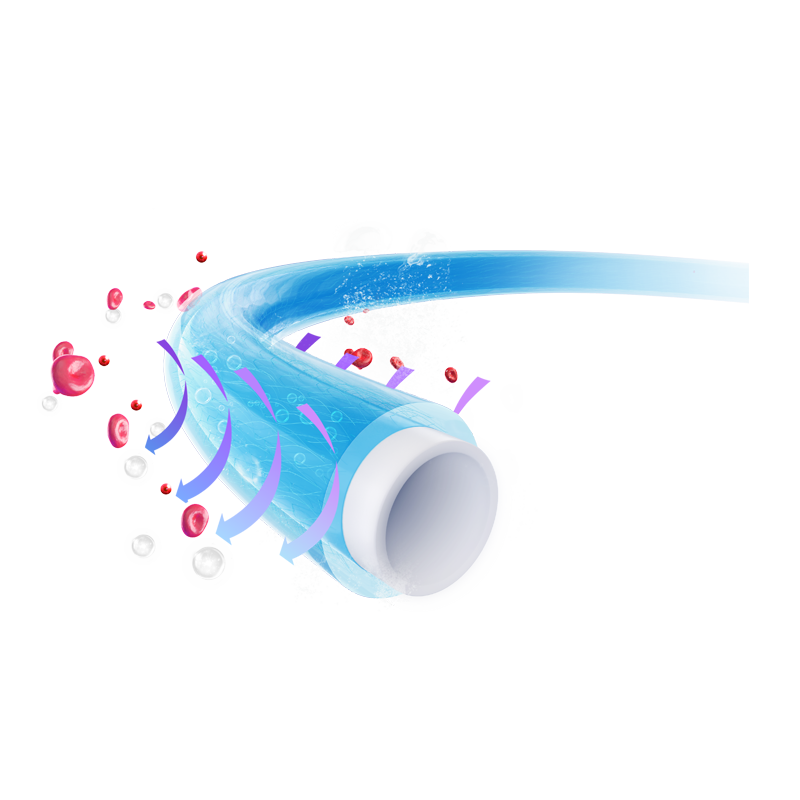
Beyond ATIII-mediated effects, heparin coatings also influence protein adsorption in ways that reduce thrombogenicity. The negative charge of heparin electrostatically repels platelets and red blood cells. Reduced fibrinogen adsorption on coated surfaces diminishes platelet adhesion and activation.
Extensive in vitro antithrombogenicity testing has been conducted. One finding has become clear: heparin coatings perform optimally under laminar flow conditions, where shear stress maintains adequate ATIII delivery to the surface.
Testing methodologies include both in vitro and in vivo approaches. In vitro tests measure markers of coagulation activation (thrombin–antithrombin complexes, fibrinopeptide A), platelet activation markers (β-thromboglobulin, PF4), and clotting times.
Platelets are critical components of thrombosis. Surface thrombogenicity correlates closely with platelet activation and consumption. Heparin coatings demonstrate excellent platelet compatibility.
The mechanism follows protein adsorption patterns. Fibrinogen adsorption promotes platelet adhesion through GPIIb/IIIa integrin binding. Von Willebrand factor adsorption enables platelet capture under high-shear conditions. Heparin coatings minimize platelet interactions by reducing the adsorption of these proteins.
The inherent properties of heparin also directly inhibit platelet interactions. The negatively charged surface generates electrostatic repulsion of platelet membranes. Platelet agonists near the surface are neutralized. Circulating platelets are preserved rather than activated and consumed.
Clinical evidence supports these platelet-sparing effects. Studies comparing heparin-coated and uncoated cardiopulmonary bypass circuits demonstrate reduced platelet consumption, lower platelet activation markers, and decreased transfusion requirements in the heparin-coated groups.
The practical implication: patients undergoing surgery with heparin-coated devices typically require fewer platelet transfusions and experience fewer bleeding complications.
Blood–device interactions trigger inflammatory responses that extend well beyond coagulation. The complement system is readily activated on foreign surfaces. Heparin coatings have shown beneficial effects in this regard.
Complement activation can proceed through three pathways: the classical pathway (antibody-dependent), the lectin pathway (mannose-binding lectin-dependent), and the alternative pathway (spontaneous C3 hydrolysis-dependent). All three pathways converge on C3 convertase formation, ultimately leading to membrane attack complex assembly.
Heparin and heparan sulfate inhibit complement activation through multiple mechanisms. The highly sulfated polysaccharide backbone binds complement components and regulatory factors. C1 inhibitor binding is enhanced. C3 convertase formation is disrupted. Membrane attack complex assembly is inhibited at multiple sites.
Clinically, reduced complement activation translates to decreased post-operative inflammation. Patients benefit from an attenuated systemic inflammatory response — potentially reducing fever, capillary leak, and organ dysfunction.
Device-related infections represent a major source of morbidity and healthcare costs. Heparin coatings provide potential anti-infective properties through both direct and indirect mechanisms.
The indirect mechanism relates to thrombosis reduction. Protein-rich thrombotic matrices support bacterial colonization and biofilm formation. Staphylococcal species readily adhere to thrombotic surfaces. By reducing thromb formation, heparin coatings indirectly lower infection risk.
Direct antimicrobial mechanisms have also been proposed. The negative charge of heparin may repel bacteria with similarly charged membranes. Some evidence suggests heparin may interfere with bacterial adhesion to host cells.
Clinical studies have documented reduced infection rates with heparin-coated devices. Hemodialysis catheters with heparin coatings show lower bloodstream infection rates compared to uncoated controls. Central venous catheter studies have shown similar trends.
ECMO provides prolonged cardiopulmonary support for critically ill patients. Blood circulates through an extracorporeal circuit for days to weeks, placing exceptional demands on blood compatibility.
Thrombotic complications in ECMO are common and potentially catastrophic. Circuit thrombosis can lead to device failure, while thromboembolic events can cause stroke or end-organ ischemia. Systemic anticoagulation is necessary but increases bleeding risk.
Heparin-coated ECMO circuits reduce circuit thrombotic complications and may enable reduced systemic anticoagulation. Clinical practice has shifted markedly toward the use of heparin-coated circuits.
What most people don't realize: circuit thrombosis is only part of the problem. Patient-side thrombosis — in the ventricles, the vasculature, pre-existing clots mobilized by the circuit — also occurs. Heparin coatings help address both issues by reducing circuit-related thrombotic activation.
The jHemo PC® platform has been validated for the demanding flow and pressure conditions of extracorporeal circulation. Coating quality translates directly into clinical practice — fewer circuit changes, fewer bleeding complications, and potentially better patient outcomes.
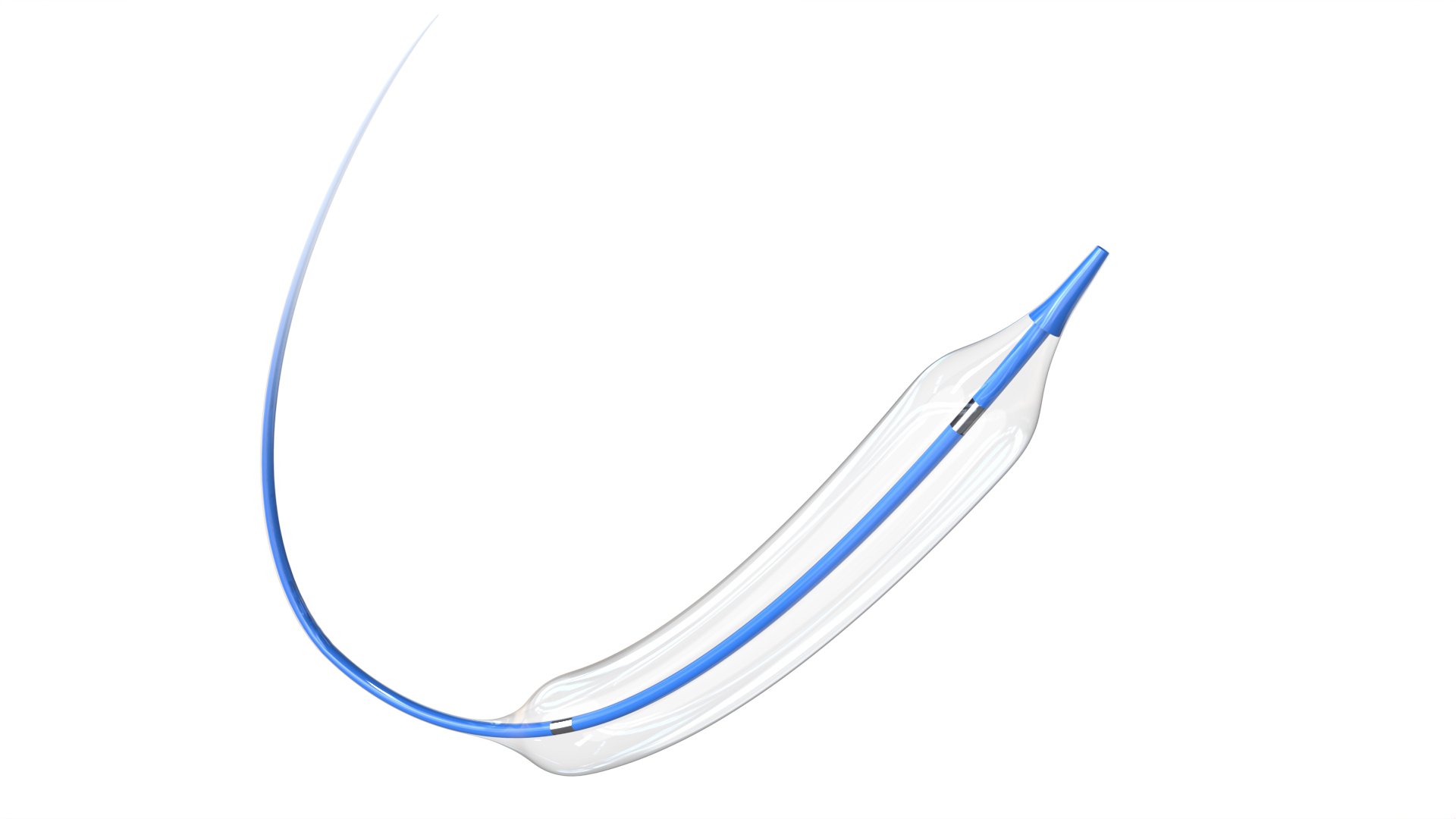
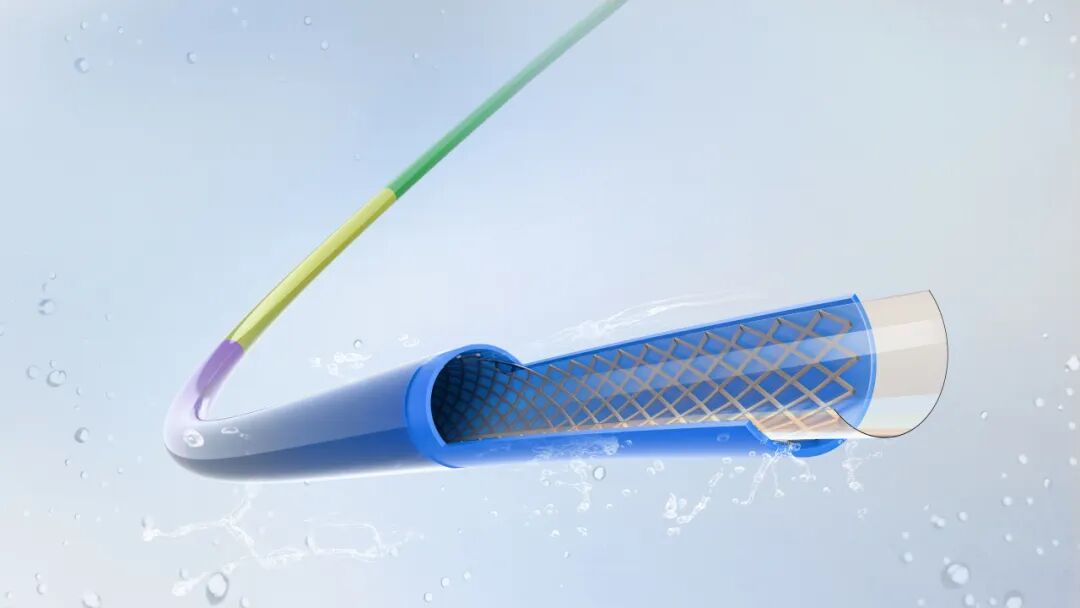
Vascular grafts and stents address occlusive and aneurysmal disease in the arterial and venous systems. Surface modification with heparin has become standard for many of these device categories.
Early vascular grafts — particularly expanded polytetrafluoroethylene (ePTFE) and Dacron prostheses — suffered from acute and subacute thrombosis, limiting clinical success rates. Heparin-coated grafts have demonstrated improved patency rates, especially in small-diameter and high-flow settings.
Drug-eluting stents combine a heparin base coating with antiproliferative drug release to address both acute thrombosis and neointimal hyperplasia. The metallic stent platform provides mechanical support, the heparin coating provides antithrombotic protection during healing, and the drug suppresses excessive neointimal formation.
Stents and grafts for peripheral artery disease benefit significantly from heparin coating, given the high thrombotic burden in the peripheral circulation. Clinical studies have documented improved primary patency rates and reduced re-intervention requirements.
Central venous catheters (CVCs) are among the most frequently placed blood-contacting devices. Thrombotic and infectious complications of CVCs are serious.
Catheter-related thrombosis — fibrin sheath formation and mural thrombus along the catheter surface — occurs in the majority of patients with long-term catheterization. These thrombi serve as infection niduses, compromise catheter function, and can lead to pulmonary embolism.
Heparin-coated catheters have demonstrated reduced thrombotic complications. Decreased fibrin sheath formation, fewer catheter occlusions, and reduced thrombotic events have been documented. Clinical experience supports the use of heparin coatings in both short-term and long-term catheters.
Ventricular assist devices (VADs) provide mechanical circulatory support for patients with advanced heart failure. These implantable pumps contact blood for weeks to months. The blood compatibility requirements are extreme.
Thrombosis on VAD surfaces can lead to device failure, pump stall, and catastrophic hemodynamic compromise. Thromboembolic events can cause stroke and end-organ ischemia. The consequences are severe, and patient management is challenging.
Heparin coatings provide an additional layer of thrombosis protection and may enable reduced intensity of systemic anticoagulation. Several contemporary VAD systems incorporate heparin-coated blood-contacting surfaces into their design. Heparin coating provides an additional safety margin for VAD patients.
Phosphorylcholine (PC) coating represents a distinct approach worth comparing. While both aim to reduce thrombosis, their mechanisms differ substantially.
PC is a zwitterionic phospholipid head group — the predominant component of the outer leaflet of cell membranes. PC coatings create surfaces that mimic natural cell membranes, reducing recognition and activation at the device surface.
How should you choose? Heparin coatings are appropriate for applications requiring active anticoagulation — high thrombotic risk, prolonged exposure, or patients with hypercoagulable states. PC coatings suit lower-risk scenarios. The decision should be based on the specific requirements of the medical device.
Surface modification strategies fall into two broad categories: bioactive (actively modifying biological responses) or passive (reducing triggers for biological responses).
Bioactive surfaces include heparin coatings, thrombomodulin coatings, nitric oxide-releasing coatings, and enzyme-based coatings. These surfaces provide active biological functionality.
Passive surface strategies focus on reducing initial protein adsorption and cell adhesion. Methods include hydrogels, PEGylation, superhydrophobic surfaces, and biomimetic phospholipid coatings.
The optimal approach depends on the specific application. High-risk, long-term devices generally benefit from active anticoagulation strategies. Combination approaches — active anticoagulation plus passive fouling resistance — provide the most comprehensive blood compatibility solutions.
Recognizing that no single surface modification addresses all aspects of blood compatibility, researchers and manufacturers have developed combination approaches.
Common combinations include:
• Heparin + Phosphorylcholine — Active anticoagulation plus passive protein resistance
• Heparin + Drug elution — Antiproliferative or anti-inflammatory drugs combined with anticoagulant coatings
• Heparin + Endothelialization promoters — Surfaces that promote endothelial cell growth for long-term integration
• Multi-layer coatings — Stacked functional layers for complex surface properties
Combination approaches are especially relevant for devices with challenging thrombotic profiles — small-diameter vascular grafts, mechanical circulatory support, and long-term implants. The ability to tailor surface properties to specific clinical needs represents the future direction of blood compatibility technology.
Blood-contacting devices must maintain coating integrity under physiological and pathological flow conditions. Shear stress can challenge coating adhesion and potentially cause delamination.
Heparin coatings must withstand a range of shear conditions. Cardiac output generates peak shear stresses of approximately 40 dynes/cm² in the aorta. Peripheral arteries experience even higher peak shear. The venous system experiences lower shear, but venous valves create turbulent flow regions.
Ionic heparin coatings are particularly susceptible to shear-induced delamination due to the reversibility of electrostatic bonding. Under high-shear conditions, heparin molecules may be stripped from the surface, especially in turbulent flow regions.
Covalently bound heparin, particularly with endpoint attachment, demonstrates superior shear resistance. Testing under simulated physiological shear conditions has confirmed coating stability.
Medical devices must be sterilized prior to implantation or use. Sterilization processes can challenge coating stability and bioactivity.
Standard sterilization methods include:
• Steam sterilization — Autoclaving at elevated temperature and pressure — challenging for many coatings due to thermal degradation
• Ethylene oxide (EtO) — Gas sterilization at lower temperatures — generally compatible with heparin coatings
• Gamma radiation — High-energy irradiation — may cause oxidative degradation of heparin
• Electron beam — An alternative radiation method similar to gamma irradiation
Heparin coatings are generally compatible with EtO sterilization, the most commonly used method for implantable devices. Gamma irradiation may be acceptable for certain coatings but requires validation.
jMedtech works with device manufacturers to verify coating performance through the intended sterilization process.
For long-term implants, coating bioactivity must persist throughout the service life. This requirement is particularly challenging for heparin coatings, as heparin is inherently susceptible to degradation.
Covalent attachment significantly enhances coating durability compared to ionic alternatives. Endpoint attachment preserves heparin chain integrity, maintaining the molecular configuration required for ATIII binding and coagulation factor inhibition.
Accelerated aging protocols expose coatings to elevated temperature conditions that accelerate degradation kinetics, enabling prediction of long-term stability. Clinical evidence supporting sustained performance continues to grow.
Heparin-coated devices must demonstrate biocompatibility through the ISO 10993 testing framework — the international standard for biological evaluation of medical devices.
Key tests for blood-contacting devices include:
• Cytotoxicity — Assessment of potential local cytotoxic effects
• Sensitization — Evaluation of potential allergic or hypersensitivity responses
• Irritation — Assessment of local tissue reactions at the implantation site
• Acute systemic toxicity — Evaluation of potential harmful systemic effects
• Hemocompatibility — Testing of effects on blood cells and coagulation, including thrombogenicity testing, hemolysis assessment, complement activation, and platelet and leukocyte counts and function
The ISO 10993-4 standard specifically addresses hemocompatibility testing, providing standardized methods for evaluating blood–device interactions.
The FDA has issued specific guidance on anticoagulant device coatings, recognizing the unique considerations for these surface modifications.
Key FDA expectations include:
• Demonstration of coating effectiveness through appropriate testing
• Characterization of coating durability and bioactivity over the intended device service life
• Assessment of systemic effects from any coating components
• Appropriate clinical validation for high-risk applications
• Clear identification of the coating and its intended function
FDA guidance emphasizes validated test methods and appropriate endpoints. Manufacturers working with jMedtech benefit from the company's experience with regulatory requirements across global markets.
Heparin-induced thrombocytopenia is a potential safety concern. HIT is an immune-mediated adverse reaction characterized by thrombocytopenia and paradoxical thrombosis.
Type II HIT involves antibodies against platelet factor 4–heparin complexes. These antibodies activate platelets through Fc receptor binding, causing thrombocytopenia and potentially severe arterial and venous thrombosis.
The incidence with systemically administered heparin varies by patient population, ranging from less than 0.1% to several percent. The risk with surface-bound heparin is theoretically lower due to minimal systemic exposure.
Patients with known HIT antibodies should not receive heparin-coated devices. Clinical monitoring may be appropriate for high-risk populations.
The jHemo PC® platform has been validated through extensive testing, demonstrating superior hemocompatibility across multiple parameters.
Validated substrate materials include:
Material Category | Specific Materials | Coating Compatibility |
Polymers | PTFE, PEBAX, Nylon, Polycarbonate | Fully validated |
Metals | Stainless steel, Nitinol, Cobalt-chromium alloys | Fully validated |
Ceramics | Alumina, Zirconia | Validated |
Composites | Fiber-reinforced polymers | Application-dependent |
The coating process is compatible with standard manufacturing workflows. jMedtech's technical team works with customers to optimize coating application for specific device geometries and production requirements.
Heparin coating technology has evolved from a promising concept to an established standard for blood-contacting medical devices. Its scientific principles are well understood, manufacturing processes have reached commercial scale, and substantial clinical evidence supports its efficacy across a wide range of device types. From ECMO circuits to vascular stents to central venous catheters, heparin coatings have demonstrated significant value in reducing thrombotic complications and improving patient outcomes.
For device manufacturers, the choice of coating technology requires consideration of device type, intended use, regulatory pathway, and production requirements. Partnering with an experienced coating partner accelerates development and mitigates risk — from material selection to process optimization to regulatory submission.
As medical devices continue to push boundaries in complexity, duration, and clinical application, the importance of effective thrombosis protection will only increase. Heparin coating technology — backed by decades of research, clinical experience, and continuous innovation — remains a cornerstone of surface modification strategies for blood-contacting devices.
Think of it this way: a heparin-coated surface functions like a dedicated cleanup crew at the blood–device interface. Surface-bound heparin captures circulating antithrombin III (ATIII), and this complex rapidly neutralizes thrombin and Factor Xa — the key enzymes in the coagulation cascade. This creates a localized anticoagulant effect at the device surface rather than a systemic one. As long as the coating remains intact and active, this protection persists.
Here is how we think about it: heparin coating functions like an active defense system, while PC coating acts more like a passive shield. For high thrombotic risk applications, long-term implants, or situations requiring active anticoagulation, choose heparin coating. For lower-risk applications where a passive approach is sufficient and cost is a consideration, PC coating may be the appropriate choice. The right decision depends on your device, patient population, and clinical requirements. At jMedtech, we work with customers to determine the optimal approach on a case-by-case basis.
The evidence is substantial and spans multiple device categories. Cardiac surgery studies (CPB and ECMO circuits) show reduced circuit thrombotic complications. Vascular graft studies demonstrate improved patency rates, particularly in small-diameter vessels. Central venous catheter studies show reduced bloodstream infections and thrombotic events. The FDA and global regulatory bodies have cleared numerous heparin-coated devices, reflecting broad acceptance of the technology in clinical practice.
This question comes up frequently, and it is a legitimate concern. Compared to systemic heparin, surface-bound heparin carries a theoretically lower risk because systemic exposure is minimal. However, we recommend against using heparin-coated devices in patients with known HIT history or existing HIT antibodies. For patients without known HIT risk, heparin-coated devices have been used with an extensive safety record, and the HIT risk appears to be very low.
For covalently bonded coatings — which we strongly recommend for long-term applications — bioactivity is maintained throughout the typical device service life. We have validated this through accelerated aging studies and long-term implantation studies. Ionic coatings are a different matter — they may gradually lose activity as heparin elutes from the surface. Covalently bonded coatings, particularly those using endpoint attachment methods, can maintain activity for months to years under physiological conditions, depending on the specific application.