The medical device industry is undergoing profound changes: all parties in the supply chain are striving to shorten product launch cycles, while product development complexity continues to increase and industry regulatory standards are becoming increasingly stringent. Original equipment manufacturers (OEMs) are under significant pressure and are increasingly inclined to rely on contract development and manufacturing organizations (CDMOs) to break down the barriers across the entire chain from R&D concept to commercialization.
A medical device CDMO is essentially a one-stop-shop for product development and manufacturing. jMedtech, for instance, handles everything from early feasibility studies and design engineering through clinical production, regulatory submission support, and scalable commercial manufacturing. That's the full value chain.
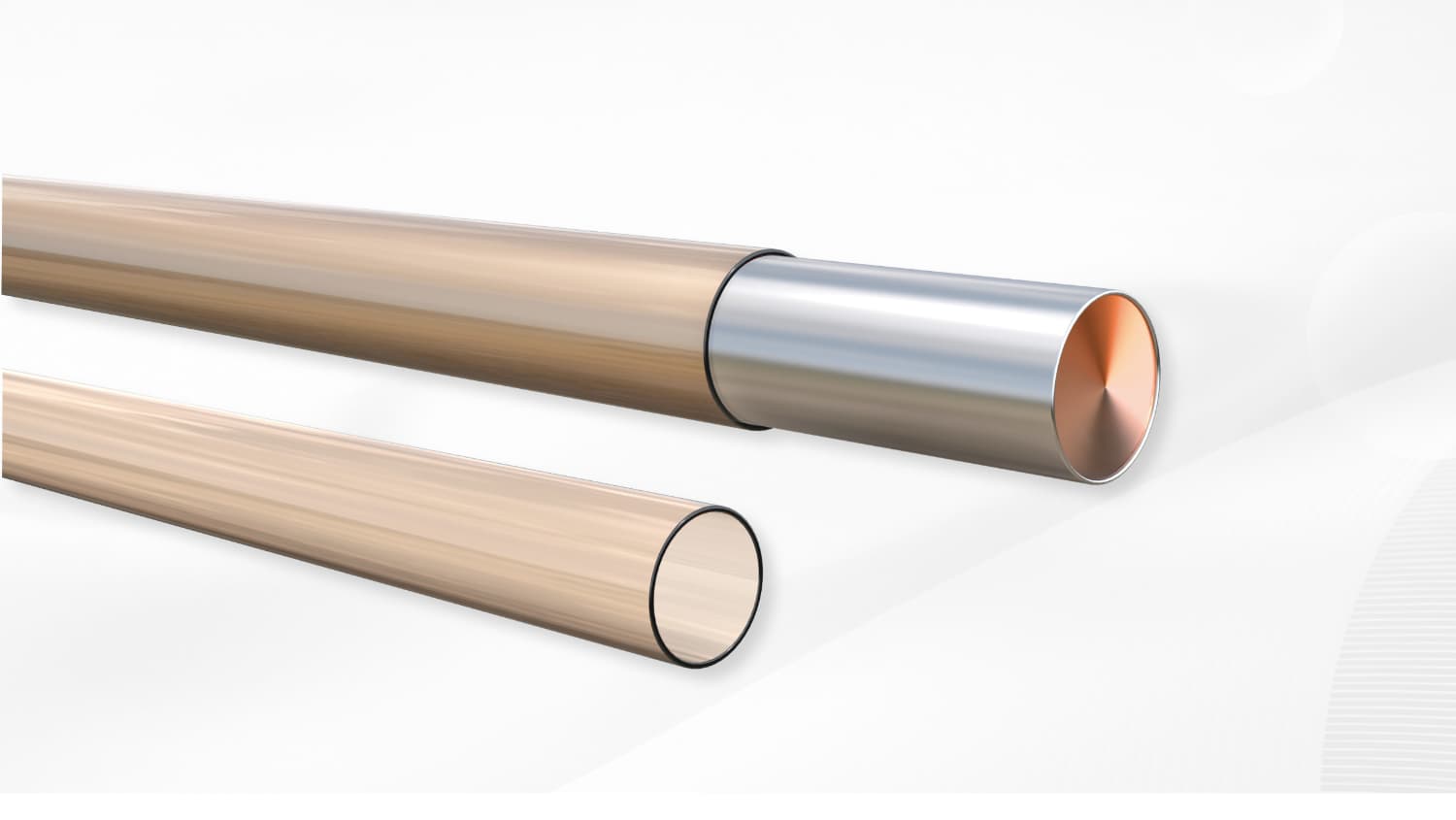
The rapid adoption of the CDMO (Contract Development and Manufacturing Organization) model is primarily due to the technological complexity of medical devices, which has exceeded the internal capabilities of many original equipment manufacturers (OEMs). Modern interventional cardiovascular devices integrate precision extruded polymer tubing, braided composite tubing, microcatheters, guiding catheters, functional coatings, catheter assembly systems, and electronic components. While individual component production is not the main challenge, the biggest hurdle lies in coordinating and managing multiple suppliers. OEMs, dealing with numerous component suppliers, are highly susceptible to communication barriers, quality control issues, and project delays. Choosing an integrated CDMO partner avoids these problems at their source.
Here's where people get confused. Let me break it down simply:
Model | Scope | Ownership | Typical Use Case |
CDMO | Development + Manufacturing | OEM retains IP | Complex devices requiring custom engineering |
CMO | Manufacturing Only | OEM provides design | High-volume production of established designs |
ODM | Design + Manufacturing (off-the-shelf) | Supplier owns design | Standardized products with minor customization |
A CDMO owns the process—the tooling, process parameters, and validated methods—while you (the OEM) keep the intellectual property over your product design. This structure lets you leverage the CDMO's engineering expertise without giving up your proprietary rights.
A CMO is more like a toll manufacturer. They execute prints and specifications you provide. No design optimization, no engineering contribution.
An ODM (Original Design Manufacturer) maintains ownership of reference designs that multiple customers can customize. Fine for commoditized products. But for highly specialized medical devices where your regulatory clearance references specific product architectures? This model doesn't work.
We've seen clients struggle for months before realizing they needed a CDMO. Here's what to look for:
• New product development with complex subsystem integration — Your device combines composite tubing, braided reinforcement structures, microcatheters, guiding catheters, polymer tubing, metal components, coatings, and electronics. You need one engineering team that understands how all these pieces interact.
• Limited internal manufacturing capabilities — Startups and mid-size OEMs often lack the investment in precision extrusion, braiding, catheter assembly, or coating infrastructure needed for complex devices like microcatheters, braided tubing, or composite catheter systems.
• Accelerated timelines to market — jMedtech's rapid prototype program delivers functional prototypes within 7 days. Seven days. That's not a typo.
• Regulatory submissions requiring validated processes — CDMOs with documented quality systems (ISO 13485) provide ready-audit evidence packages that strengthen 510(k) and PMA submissions.
• Scalability concerns — Commercial launch volumes often exceed prototype-scale production by orders of magnitude. A CDMO with proven scale-up track records mitigates this risk significantly.
Every CDMO engagement follows a structured lifecycle. Each phase builds on deliverables from the previous stage. Understanding this progression helps you plan resource allocation, set realistic timelines, and define clear acceptance criteria for each gate.
The lifecycle starts with a Feasibility Assessment evaluating technical, commercial, and regulatory viability. During this phase, you and the CDMO jointly define:
• Target device specifications
Dimensions, material requirements, performance thresholds
• Production volume projections
Prototype quantities, clinical batch sizes, commercial forecast
• Regulatory pathway
510(k), De Novo, PMA, or international equivalents (CE Mark under MDR)
• Cost targets
Target selling price, acceptable margin structure, total cost of ownership
Design and development covers all engineering activities transforming product specifications into production-ready documentation. Key deliverables include:
• Engineering drawings with GD&T (Geometric Dimensioning and Tolerancing) per ASME Y14.5 standards
• Material specifications and approved supplier lists (ASLs)
• Process flow diagrams and process failure mode effects analysis (PFMEA)
• Design verification protocols and acceptance criteria
• Risk management files per ISO 14971
During D&D, the CDMO's process engineering team works closely with your design team to optimize the device architecture for manufacturability. This is where Design for Manufacturing (DFM) principles directly impact your commercial viability.
Let me give you a real example. A catheter hub assembly that's easy to assemble manually may require expensive automated equipment at 100,000-unit annual volumes. Conversely, a design optimized for high-speed automation may be impossible to prototype without specialized equipment. The tradeoff depends entirely on your volume projections—and you need to make that call early.
Design transfer formalizes the transition from development to production. This critical phase converts design intent into production documentation, validates manufacturing processes, and establishes the infrastructure for repeatable commercial output.
Poor design transfer is among the leading causes of launch delays and quality escapes. We've seen clients lose six months of development time because design transfer was treated as an afterthought. For products like braided guiding catheters or composite microcatheters—where braid integration, tip geometry, and liner adhesion must be replicated consistently from prototype to full production—this phase is non-negotiable. Investing in a rigorous transfer protocol protects both your timeline and—more importantly—patient safety.
The commercial manufacturing phase kicks in after successful validation and regulatory clearance. Key considerations:
• Production scheduling aligned with customer forecast and inventory targets
• Change control processes governing specification modifications
• Continuous improvement initiatives targeting yield optimization and cost reduction
• Supply chain resilience with multi-source material strategies where appropriate
Design for Manufacturing is all about optimizing product designs for efficient, repeatable, cost-effective production—without compromising device performance or safety. In medical devices, DFM carries extra weight because design changes after validation require regulatory re-assessment. That's a substantial cost and timeline hit.
Material selection is one of the most consequential DFM decisions. Your polymer or metal must satisfy mechanical requirements, biostability demands, AND sterilization compatibility simultaneously. Common selection criteria:
• Mechanical properties
Tensile strength, flexural modulus, and durometer hardness must match the device's intended use environment.
• Chemical resistance
Devices sterilized by EtO (ethylene oxide) or gamma irradiation must resist property degradation from repeated exposure.
• Biocompatibility
Materials must pass ISO 10993 biocompatibility testing. Pay particular attention to cytotoxicity, sensitization, and irritation endpoints.
• Radiopacity
If your device requires visibility under fluoroscopy, radiopaque fillers (barium sulfate, tungsten, platinum iridium) may be specified. These impact processing conditions.
Precision tolerance control sets medical device manufacturing apart from most industrial sectors. Dimensional requirements of ±0.0003" (7.6 μm) are common in catheter liner and small-bore tubing applications. Achieving these tolerances requires:
• In-process gauging using laser micrometers, optical comparators, and coordinate measuring machines (CMMs)
• Process capability analysis expressed as Cpk (Process Capability Index), with medical device processes typically requiring Cpk ≥ 1.33 for critical characteristics
• Tooling maintenance protocols specifying inspection frequency and replacement criteria
Device architectures that seem straightforward in prototype reveal assembly bottlenecks at commercial volumes. This is especially true for multi-component assemblies like braided composite catheters—where braid placement, reflow bonding, and tip forming must happen in precise sequence—or guiding catheters that integrate PTFE liners, braid reinforcement, and polymer jackets into a single unified shaft. Microcatheters present their own challenges: extremely small lumen dimensions demand specialized handling fixtures and near-zero tolerance for misalignment during tip bonding. DFM analysis should evaluate:
• Number of components
Each additional part introduces handling time, potential for mis-assembly, and supply chain complexity.
• Access constraints
Features requiring reach-through or awkward positioning multiply assembly cycle times.
• Orientation sensitivity
Parts that must be assembled in a specific orientation require indexing or dedicated fixtures.
• Joining methods
Adhesive bonding, ultrasonic welding, thermal fusion, and mechanical fastening each carry distinct process windows and quality verification requirements.
Design transfer converts a validated prototype design into a commercial manufacturing process. It's often described as the highest-risk phase of medical device development.
Studies indicate that 40-60% of medical device recalls trace back to design transfer deficiencies. Production processes failing to consistently reproduce design intent—that's where things go wrong.
Initial design transfer begins with prototype production using development-grade documentation. At this stage, the CDMO produces units under a controlled but less rigid quality system environment—sometimes called "prototype QA"—allowing faster iteration while maintaining traceability.
Deliverables:
• First Article Inspection (FAI) reports comparing prototype dimensions to design intent
• Preliminary process capability studies (Cpk pilot runs)
• Material lot traceability records for all components
• Identification of process parameters requiring further optimization
Clinical production requires a fully compliant quality system environment. All production follows documented procedures with complete traceability from raw material lot to finished device.
Critical activities:
• IQ/OQ/PQ validation of all critical processes
• First article inspection using statistically representative sample sizes (typically n=30 minimum)
• Sterilization validation if the device will be sterilized (EtO, gamma, steam)
• Shelf-life validation planning for device storage stability studies
Clinical batches also serve as the basis for process performance qualification (PPQ)—the integrated confirmation that all processes, operating within their validated ranges, consistently produce devices meeting all specifications.
Commercial transfer formalizes the production relationship and establishes operational infrastructure for sustained manufacturing.
Key elements:
• Approved Process Parameters documented in device history records (DHRs)
• Updated PFMEA reflecting any process parameter adjustments made during validation
• Quality Agreement defining OEM and CDMO responsibilities (detailed in the Regulatory Compliance section)
• Production introduction plan with volume ramp schedule and acceptance criteria
Production yields at commercial scale typically start 10-20% below validation batch yields. Operators develop muscle memory. Process engineers refine edge-of-envelope parameters. Building this learning time into your commercial launch plan prevents quality escapes and schedule pressure.
Pitfall | Consequence | Mitigation |
Incomplete specification documentation | Production produces to incorrect tolerances | Comprehensive specification review checklist |
Unvalidated critical processes | Quality escapes at commercial scale | Mandatory PQ completion before first commercial order |
Inadequate tooling transfer | Dimensional drift post-transfer | Tool qualification protocols with dimensional baselines |
Missing supplier qualification data | Regulatory audit findings | Sub-tier supplier audit trail documentation |
Unclear acceptance criteria | Dispute over first article approval | Pre-defined acceptance criteria in Quality Agreement |
Process validation is the documented evidence that a process consistently produces a product meeting predetermined specifications. FDA's Process Validation Guidance (2011) and ISO 13485:2016 Section 7.5 establish a three-stage framework.
IQ establishes that equipment and supporting systems are installed correctly and according to manufacturer specifications.
IQ activities include:
• Verification of equipment model numbers, serial numbers, and software versions against purchase orders
• Confirmation of utility connections (power, compressed air, nitrogen, vacuum) match equipment requirements
• Calibration records for all measurement and monitoring instruments
• Environmental qualification of the installation location (cleanroom classification, temperature, humidity ranges)
IQ is fundamentally a documentary exercise. The question it answers: "Is everything in place correctly?"
OQ demonstrates that equipment operates within specified limits under all expected conditions. This goes beyond running the machine at its "happy path" setting.
OQ protocols must test:
• Upper and lower operating limits — The equipment must produce acceptable product when process parameters are at their extreme acceptable values, not just at their nominal setting.
• Challenge conditions — Simulated disturbances (power fluctuations, material lot variations, ambient temperature extremes) verify the process remains in control.
• Safety interlocks — Emergency stops, door interlocks, and alarm systems must function correctly.
A common OQ misconception: conflating OQ with "validation testing."
OQ validates the equipment's capability to operate within defined ranges. It does not confirm that the process as a whole produces acceptable product at those conditions. That determination comes in PQ.
PQ is the final validation stage. It demonstrates that the validated process consistently produces product meeting specifications under routine production conditions.
PQ characteristics:
• Extended duration — PQ typically runs across multiple production shifts and material lots to capture real-world variation
• Statistically representative sample sizes — Typically minimum 3 lots with 30+ samples per lot for critical dimensions
• Production operators — Unlike OQ (which may use dedicated validation technicians), PQ should involve the operators who will run the process commercially
• Process signature confirmation — Cpk calculations from PQ data establish the process capability baseline against which future performance is measured
For a PTFE liner extrusion process—or a complete braided composite catheter assembly—PQ validation requires demonstrating that wall thickness (target 0.0003"/7.6 μm, tolerance ±0.0003"), concentricity (≥95%), and ovality (≥99%) meet specifications across at least three consecutive material lots and multiple production runs. For microcatheters and guiding catheters, additional acceptance criteria typically include pull force testing, tip bond strength, and dimensional consistency across the full active length.
Here's the thing about regulatory compliance: it's not a department. It's the operating infrastructure of every medical device manufacturer and CDMO.
The regulatory landscape establishes the rules of engagement. Failure to maintain compliance results in warning letters, import alerts, consent decrees—or worse.
ISO 13485:2016 is the global standard for quality management systems in medical devices. Adopted by regulatory authorities in the EU, Canada, Japan, Australia, and China. It establishes requirements for:
• Documented quality policy and quality objectives
• Management review and internal audit programs
• Resource management (personnel, infrastructure, work environment)
• Product realization (planning, design, purchasing, production, monitoring, measurement)
• Corrective and preventive action (CAPA) systems
• Traceability requirements from component to finished device
FDA 21 CFR Part 820 (the Quality System Regulation, or QSR) is the US regulatory equivalent. Aligned with ISO 13485 but with distinct documentation and reporting requirements. FDA's Quality System Inspection Technique (QSIT) provides the framework for FDA investigator audits of medical device establishments.
A Quality Agreement is a legally binding contract defining OEM and CDMO responsibilities regarding quality-related activities.
FDA guidance and EU MDR requirements emphasize that the OEM cannot delegate ultimate product accountability. But the CDMO bears specific operational responsibilities.
Essential Quality Agreement elements:
• Responsibility matrix clearly delineating who owns each quality activity (e.g., incoming inspection, in-process testing, final release testing)
• Specification ownership — Which party owns the device master record (DMR) and which controls changes to it
• Deviation and CAPA procedures — How non-conformances are identified, investigated, and resolved
• Audit rights — OEM's right to audit the CDMO, including frequency and scope
• Regulatory notification obligations — Which party notifies regulators in the event of a field action or recall
• Record retention — Duration and accessibility requirements for device history records (DHRs)
When you engage a CDMO, understand this: the CDMO's supplier network becomes an extension of your supply chain.
Supplier change control processes govern how material suppliers, sub-component manufacturers, and secondary processors are managed:
• Approved Supplier List (ASL) — Only pre-qualified suppliers may be used without explicit customer approval
• Change notification — Suppliers must notify the CDMO (and, per Quality Agreement, the OEM) of material or process changes
• Qualification requirements — Material changes may require re-validation of affected processes
• Audit programs — Critical sub-tier suppliers should be subject to periodic quality audits
Let's be honest—selecting a CDMO is one of the most consequential decisions you'll make. The partnership typically spans years. Substantial capital commitment is involved. And this decision directly impacts patient safety.
A structured evaluation framework reduces mis-selection risk.
Technical capability assessment goes beyond reviewing a capability matrix.
Evaluate:
• Process capability data — Request Cpk reports for processes similar to your requirements. A CDMO claiming ±0.0003" tolerance capability should demonstrate actual capability data, not just theoretical specifications.
• Equipment inventory — Verify that the equipment on the capability matrix is actually installed, qualified, and available. Some CDMOs list equipment they don't own or haven't qualified.
• Engineering staff qualifications — Review the CDMO's engineering team's experience in your specific device category. A CDMO experienced in orthopaedic implants may lack expertise in interventional catheter systems.
• Material compatibility databases — Ask for documented evidence of successful processing of your target materials, including sterilization history if applicable.
Cleanroom classification directly affects device safety and regulatory pathway.
Evaluate:
• Cleanroom classification — ISO 7 (Class 10,000) and ISO 8 (Class 100,000) cleanrooms are common for assembled devices. Some processes require ISO 6 (Class 1,000) or better.
• Cleanroom qualification records — Request particle count data and airflow visualization studies.
• Contamination control programs — Personnel flow, material flow, and environmental monitoring programs should be documented and validated.
• Multi-product vs. dedicated lines — Dedicated manufacturing lines reduce cross-contamination risk but increase minimum commercial commitments.
A CDMO's regulatory history is a window into its operational discipline.
Investigate:
• FDA establishment registration — Verify the CDMO is registered as a contract manufacturer (type III vs. type I establishment).
• 483 observations and warning letters — Review FDA inspection history for patterns of repeat observations.
• Notified Body audit reports — For EU-targeted products, review ISO 13485 audit findings and closure evidence.
• Customer references — Speak with current and former customers about their audit experiences and any regulatory issues encountered.
Medical device IP protection extends beyond contractual language.
Evaluate:
• Physical separation — Are dedicated manufacturing cells available for proprietary programs?
• IT security — Are production data systems segregated from other customer programs?
• Communication protocols — How does the CDMO structure program communication? Dedicated program managers, weekly status reports, and escalation procedures indicate mature program management.
• Conflict of interest provisions — Does the CDMO manufacture competing devices for other customers in the same therapeutic area?
jMedtech is a Shenzhen-based medical device CDMO specializing in precision polymer components, surface treatment coatings, and assembled catheter systems for global OEM partners. Product expertise spans PTFE liners, braided tubing, composite tubing, microcatheters, guiding catheters, steerable sheaths, and specialty coating systems. Founded with a mission to democratize access to world-class manufacturing infrastructure, jMedtech has grown from a regional supplier to a global partner serving over 600 clients across more than 30 countries.
jMedtech's greatest differentiation is its vertically integrated service model. Rather than offering discrete services, jMedtech provides a seamless development-to-manufacturing platform where the same engineering team that optimized the product design during development leads the design transfer into production. This continuity eliminates the information loss and miscommunication that frequently occur when development and manufacturing are managed by separate organizations.
The platform encompasses:
• Concept and feasibility engineering — Material selection, DFMA analysis, regulatory pathway assessment
• Prototype development — 7-day rapid prototype delivery for qualifying programs
• Design and development — Full D&D services including design verification and risk management
• Process validation — IQ/OQ/PQ execution with regulatory submission support
• Commercial manufacturing — Scale-up to high-volume production with SPC-driven quality control
The medical device CDMO partnership model represents a strategic evolution in how our industry approaches product development and manufacturing. By consolidating development engineering, process validation, and commercial production under a single accountable partner, OEMs can redirect internal resources toward core competencies—clinical development, regulatory strategy, and commercial execution—while leveraging the CDMO's specialized infrastructure and expertise.
Selecting the right CDMO requires rigorous evaluation of technical capabilities, quality systems, regulatory track record, and cultural alignment. Whether you're developing microcatheters for neurovascular intervention, braided composite tubing for steerable sheaths, or guiding catheters for cardiac procedures, the investment in a thorough selection process pays dividends throughout the commercial lifecycle. Fewer quality escapes. Shorter time-to-market. More predictable production costs.
For OEMs seeking a partner that combines the speed and flexibility of a specialist organization with the scale and infrastructure of a global manufacturer, jMedtech's integrated platform offers a compelling combination. Three ISO 13485-certified facilities. Over 600 global clients. Specialized capabilities in precision extrusion, advanced coatings, and catheter assembly.
jMedtech is positioned to serve as a true development-to-commercialization partner for the next generation of medical devices—from microcatheters and braided composite tubing to guiding catheters and steerable sheaths.
1. What is a medical device CDMO and how does it differ from a traditional contract manufacturer?
Here's the short answer: a CDMO (Contract Development and Manufacturing Organization) does both development AND manufacturing. A traditional contract manufacturer (CMO) only executes production based on designs you provide.
CDMOs bring engineering expertise, process development, and validation capabilities to the table. For complex devices requiring custom engineering and regulatory compliance, this matters—a lot. We've seen clients struggle with CMOs because the manufacturer couldn't contribute meaningfully to solving design problems that came up during development—especially when it comes to intricate products like braided composite catheters, multi-lumen microcatheters, or guiding catheters with integrated PTFE liners.
2. What criteria should I use to evaluate a CDMO's technical capabilities?
Don't just look at their capability matrix. Here's what actually matters:
First, ask for documented process capability data (Cpk reports). If they claim ±0.0003" tolerance capability, they should show you real production data, not just theoretical specs.
Second, verify their equipment through facility audits. Some CDMOs list equipment they don't actually own or haven't qualified. Check specifically for braiding machines, co-extrusion lines, and microcatheter assembly fixtures if those are relevant to your program.
Third, assess their engineering team's experience in YOUR specific device category. A track record in orthopaedic implants doesn't automatically translate to interventional catheter expertise.
Fourth, review their material compatibility databases with real production examples.
And honestly? Talk to their current customers. Not just the ones on their reference list.
3. How long does the typical CDMO engagement take from concept to commercial production?
It varies, but you're typically looking at 12-24 months from concept to commercial production. Here's the rough breakdown:
• Feasibility assessment: 2-4 weeks
• Design and development: 3-6 months
• Design transfer and validation: 3-8 months
• Regulatory submission review: 3-12 months (depends heavily on your pathway)
Some CDMOs like jMedtech offer accelerated prototype programs that deliver functional prototypes within 7 days. That's a game-changer if you're trying to derisk early design decisions.
But let me be upfront: the regulatory review timeline is often the wild card. Plan conservatively.
4. What quality system standards must a medical device CDMO maintain?
At minimum: ISO 13485 certification. That's the foundational quality management system standard.
For US market access: FDA 21 CFR Part 820 (Quality System Regulation) compliance is required.
For EU market access: conformity assessment per the EU Medical Device Regulation (MDR 2017/745).
Beyond these, be prepared for customer-specific requirements from major healthcare systems and group purchasing organizations. These vary and can add complexity to your quality system documentation.
5. How does a Quality Agreement protect my company's intellectual property and product quality?
A Quality Agreement formally defines who owns what. Design ownership. Change control procedures. Deviation management. Audit rights. Regulatory notification obligations.
It ensures YOU retain control over device specifications and design changes while the CDMO commits to validated processes and quality standards.
The agreement should explicitly address IP protection, sub-tier supplier management, and record retention. Read the fine print. Actually read it. We've seen clients surprised by terms they didn't catch during negotiation.
A well-structured Quality Agreement isn't about distrust. It's about clarity. When everyone knows their responsibilities, projects run smoother and disputes are resolved faster.